
Facts you should know about cervical cancer
Overview
Globally, cervical cancer is the fourth most common cancer in women, with 604 000 new cases in 2020. About 90% of the 342 000 deaths caused by cervical cancer occurred in low- and middle-income countries. The highest rates of cervical cancer incidence and mortality are in sub-Saharan Africa (SSA), Central America and South-East Asia. Regional differences in the cervical cancer burden are related to inequalities in access to vaccination, screening and treatment services, risk factors including HIV prevalence, and social and economic determinants such as sex, gender biases and poverty. Women living with HIV are 6 times more likely to develop cervical cancer compared to the general population, and an estimated 5% of all cervical cancer cases are attributable to HIV. The contribution of HIV to cervical cancer disproportionately affects younger women, and as a result, 20% of children who lose their mother to cancer do so due to cervical cancer.
Causes
Human papillomavirus (HPV) is a common sexually transmitted infection which can affect the skin, genital area and throat. Almost all sexually active people will be infected at some point in their lives, usually without symptoms. In most cases the immune system clears HPV from the body. Persistent infection with high-risk HPV can cause abnormal cells to develop, which go on to become cancer.
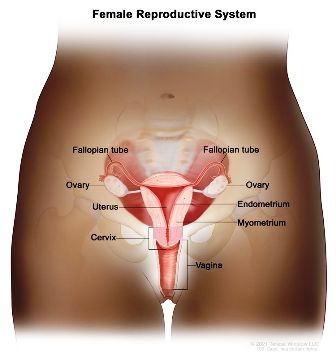
Persistent HPV infection of the cervix (the lower part of the uterus or womb, which opens into the vagina – also called the birth canal) if left untreated, causes 95% of cervical cancers. Typically, it takes 15–20 years for abnormal cells to become cancer, but in women with weakened immune systems, such as untreated HIV, this process can be faster and take 5–10 years. Risk factors for cancer progression include the grade of oncogenicity of the HPV type, immune status, the presence of other sexually transmitted infections, number of births, young age at first pregnancy, hormonal contraceptive use, and smoking.
Prevention
Boosting public awareness, access to information and services are key to prevention and control across the life course.
- Being vaccinated at age 9–14 years is a very effective way to prevent HPV infection, cervical cancer and other HPV-related cancers.
- Screening from the age of 30 (25 years in women living with HIV) can detect cervical disease, which when treated, also prevents cervical cancer.
- At any age with symptoms or concerns, early detection followed by prompt quality treatment can cure cervical cancer.
HPV vaccination and other prevention steps
As of 2023, there are 6 HPV vaccines available globally. All protect against the high-risk HPV types 16 and 18, which cause most cervical cancers and have been shown to be safe and effective in preventing HPV infection and cervical cancer.
As a priority, HPV vaccines should be given to all girls aged 9–14 years, before they become sexually active. The vaccine may be given as 1 or 2 doses. People with reduced immune systems should ideally receive 2 or 3 doses. Some countries have also chosen to vaccinate boys to further reduce the prevalence of HPV in the community and to prevent cancers in men caused by HPV.
Other important ways to prevent HPV infection include:
- being a non-smoker or stopping smoking
- using condoms
- voluntary male circumcision.
Cervical screening and treatment of precancers
Women should be screened for cervical cancer every 5–10 years starting at age 30. Women living with HIV should be screened every 3 years starting at age 25. The global strategy encourages a minimum of two lifetime screens with a high-performance HPV test by age 35 and again by age 45 years. Precancers rarely cause symptoms, which is why regular cervical cancer screening is important, even if you have been vaccinated against HPV.
Self-collection of a sample for HPV testing, which may be a preferred choice for women, has been shown to be as reliable as samples collected by healthcare providers.
After a positive HPV test (or other screening method) a healthcare provider can look for changes on the cervix (such as precancers) which may develop into cervical cancer if left untreated. Treatment of precancers is a simple procedure and prevents cervical cancer. Treatment may be offered in the same visit (the see and treat approach) or after a second test (the see, triage and treat approach), which is especially recommended for women living with HIV.
Treatments of precancers are quick and generally painless causing infrequent complications. Treatment steps include colposcopy or visual inspection of the cervix to locate and assess the lesion followed by:
- thermal ablation, which involves using a heated probe to burn off cells;
- cryotherapy, which involves using a cold probe to freeze off the cells;
- LEETZ (large loop excision of the transformation zone), which involves removing your abnormal tissues with an electrically heated loop; and/or
- a cone biopsy, which involves using a knife to remove a cone-shaped wedge of tissue.
Early detection, diagnosis and treatment of cervical cancer
Cervical cancer can be cured if diagnosed and treated at an early stage of disease. Recognizing symptoms and seeking medical advice to address any concerns is a critical step. Women should see a healthcare professional if they notice:
- unusual bleeding between periods, after menopause, or after sexual intercourse
- increased or foul-smelling vaginal discharge
- symptoms like persistent pain in the back, legs, or pelvis
- weight loss, fatigue and loss of appetite
- vaginal discomfort
- swelling in the legs.
Clinical evaluations and tests to confirm a diagnosis are important and will generally be followed by referral for treatment services, which can include surgery, radiotherapy and chemotherapy as well as palliative care to provide supportive care and pain management.
Management pathways for invasive cancer care are important tools to ensure that a patient is referred promptly and supported as they navigate the steps to diagnosis and treatment decisions. Features of quality care include:
- a multidisciplinary team ensuring diagnosis and staging (histological testing, pathology, imaging) takes place prior to treatment decisions;
- treatment decisions in line with national guidelines; and
- interventions are supported by holistic psychological, spiritual, physical and palliative care.
As low- and middle-income countries scale-up cervical screening, more cases of invasive cervical cancer will be detected, especially in previously unscreened populations. Therefore, referral and cancer management strategies need to be implemented and expanded alongside prevention services.
- Courtesy: WHO




{kind=link}
0 Comments
No Comments Yet!
You can be first to comment this post!